Data from the National Hospital Ambulatory Medical Care Survey, 2010–2011
- In 2010–2011, the emergency department (ED) visit rate for motor
vehicle traffic injuries was highest among persons aged 16–24 years. The
rates declined with age after 16–24, with rates for those aged 0–15
similar to those 65 and over.
- The overall ED visit rate for motor vehicle traffic injuries was
higher among non-Hispanic black persons compared with non-Hispanic white
and Hispanic persons.
- Imaging services were ordered or provided at 70.2% of ED visits
for motor vehicle traffic injuries, which was higher than for other
injury-related ED visits (55.9%).
- About one-half of ED visits for motor vehicle traffic injuries had
a primary diagnosis of sprains and strains of the neck and back,
contusion with intact skin surface, or spinal disorders.
In spite of improvements in motor vehicle safety in recent years,
motor vehicle crashes remain a major source of morbidity and mortality
in the United States (
1–3).
Motor vehicle-related deaths and injuries also result in substantial
economic and societal costs related to medical care and lost
productivity (
4).
This report describes the rates and characteristics of emergency
department (ED) visits for motor vehicle traffic injuries during
2010–2011 based on nationally representative data from the National
Hospital Ambulatory Medical Care Survey (NHAMCS).
Did ED visit rates for motor vehicle traffic injuries differ by age?
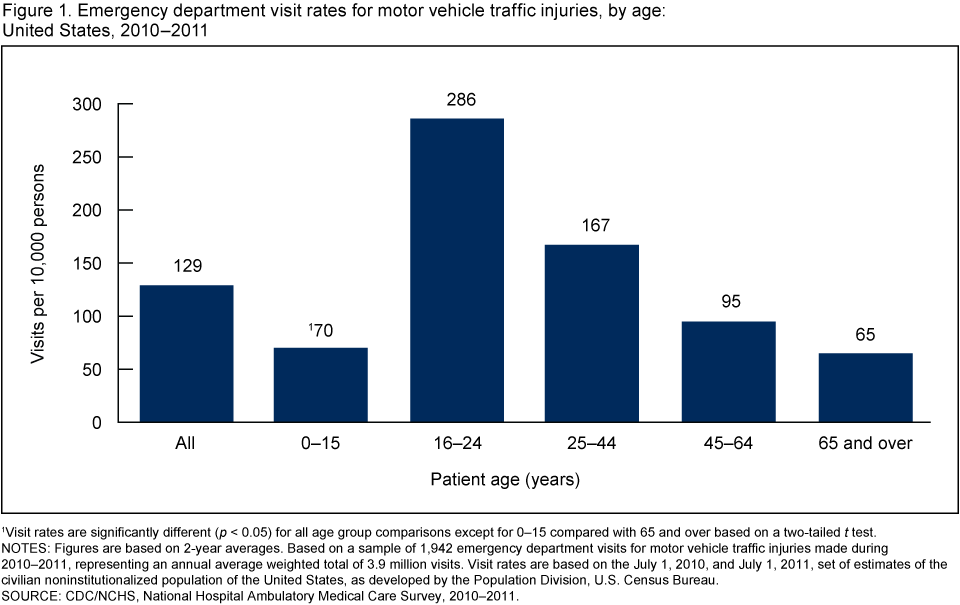
- In 2010–2011, there were an estimated 3.9 million annual average ED
visits for motor vehicle traffic injuries. The overall ED visit rate
for motor vehicle traffic injuries was 129 per 10,000 persons (Figure 1).
- The ED visit rate for motor vehicle traffic injuries was highest
among persons aged 16–24 years. The rate increased from 70 per 10,000
persons among those aged 0–15 to peak at 286 per 10,000 persons for
those aged 16–24. The rate then declined with increasing age, reaching a
rate of 65 per 10,000 persons for those aged 65 and over.
1Visit rates are significantly different (p < 0.05) for all age group comparisons except for 0–15 compared with 65 and over based on a two-tailed t test.
NOTES: Figures are based on 2-year averages. Based on a sample of 1,942
emergency department visits for motor vehicle traffic injuries made
during 2010–2011, representing an annual average weighted total of 3.9
million visits. Visit rates are based on the July 1, 2010, and July 1,
2011, set of estimates of the civilian noninstitutionalized population
of the United States, as developed by the Population Division, U.S.
Census Bureau.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2010–2011.
Did ED visit rates for motor vehicle traffic injuries differ by race and ethnicity?
- The overall ED visit rate for motor vehicle traffic injuries was
higher among non-Hispanic black persons (260 per 10,000 persons)
compared with non-Hispanic white persons (119 per 10,000 persons) and
Hispanic persons (104 per 10,000 persons) (Figure 2).
- The visit rate was higher for non-Hispanic black persons compared
with Hispanic persons for all age groups. The visit rate was higher for
non-Hispanic black persons compared with non-Hispanic white persons for
all age groups except 16–24.
- For persons aged 16–24, the visit rate was higher for non-Hispanic white persons compared with Hispanic persons.
1Visit rate for non-Hispanic black persons is significantly different (p < 0.05) from non-Hispanic white persons and Hispanic persons based on a two-tailed t test.
2Visit rate for Hispanic persons is significantly different
(p < 0.05) from non-Hispanic white persons and non-Hispanic black
persons for the age group 16–24 based on a two-tailed t test.
NOTES: Figures are based on 2-year averages. Visit rates are based on
the July 1, 2010, and July 1, 2011, set of estimates of the civilian
noninstitutionalized population of the United States, as developed by
the Population Division, U.S. Census Bureau.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2010–2011.
Did arrival by ambulance,
triage status, and hospital admission differ for motor vehicle traffic
injury ED visits compared with other injury-related ED visits?
- Ambulance was the mode of arrival for 42.9% of ED visits for
motor vehicle traffic injuries. This percentage was more than twice as
high as for other injury-related ED visits (16.6%) (Figure 3).
- In spite of more frequent arrival by ambulance, the percentage of
ED visits for motor vehicle traffic injuries with a triage status of
immediate or emergent (11.4%) was only slightly higher than for other
injury-related ED visits (8.9%).
- No statistically significant difference was observed in the
percentage of ED visits for motor vehicle traffic injuries leading to
hospital admission (5.7%) compared with other injury-related ED visits
(6.6%).
1Percentage is significantly different (p < 0.05) for motor vehicle traffic injuries compared with other causes of injury based on a two-tailed t test.
NOTE: Figures are based on 2-year averages.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2010–2011.
Did the percentage of imaging
tests ordered or provided at ED visits for motor vehicle traffic
injuries differ from other injury-related ED visits?
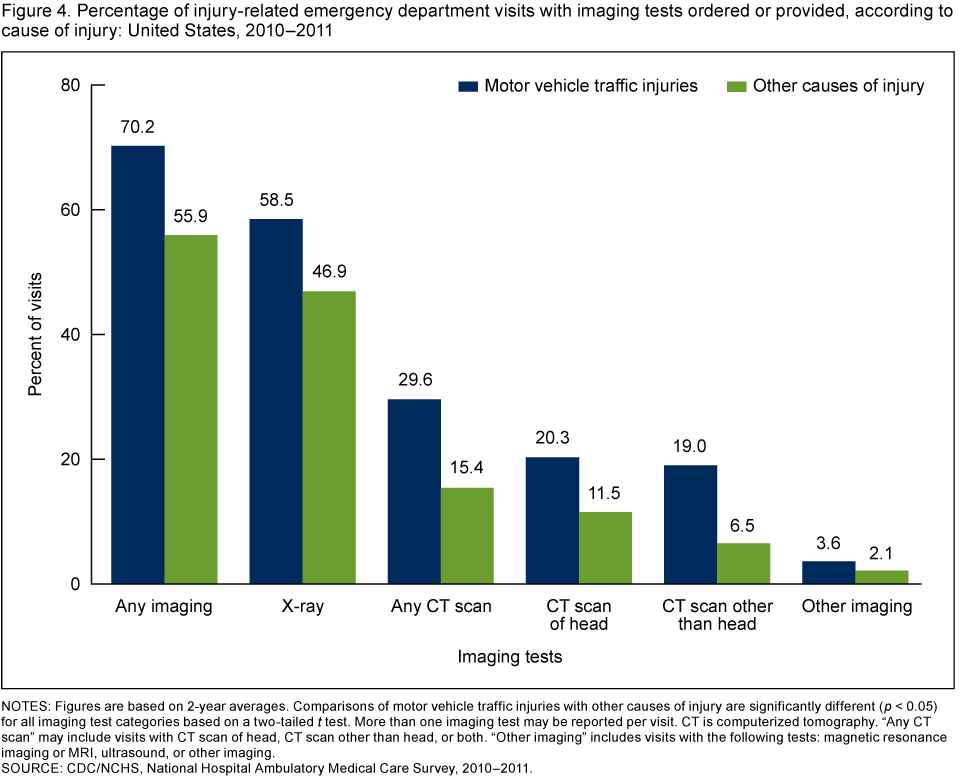
- Imaging was ordered or provided at 70.2% of ED visits for motor
vehicle traffic injuries, which was higher than for other injury-related
ED visits (55.9%) (Figure 4).
- A higher percentage of x-rays, any computerized tomography (CT)
scans, head CT scans, CT scans other than head, and other imaging were
ordered or provided at ED visits for motor vehicle traffic injuries
compared with other injury-related ED visits.
NOTES: Figures are based on 2-year averages.
Comparisons of motor vehicle traffic injuries with other causes of
injury are significantly different (p < 0.05) for all imaging test categories based on a two-tailed t
test. More than one imaging test may be reported per visit. CT is
computerized tomography. "Any CT scan" may include visits with CT scan
of head, CT scan other than head, or both. "Other imaging" includes
visits with the following tests: magnetic resonance imaging or MRI,
ultrasound, or other imaging.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2010–2011.
What were the leading primary
diagnoses associated with ED visits for motor vehicle traffic injuries?
Did these differ from other injury-related ED visits?
- Sprains and strains of the neck and back (23.6%) was the leading
primary diagnosis associated with ED visits for motor vehicle traffic
injuries, followed by contusion with intact skin surface (15.2%) and
then spinal disorders (8.0%) (Figure 5).
These diagnoses, along with observation and evaluation for suspected
conditions not found (5.4%), were more likely to be made at ED visits
for motor vehicle traffic injuries compared with other injury-related ED
visits.
- Sprains and strains excluding neck and back (6.5%), fractures
(6.1%), and open wounds (3.7%) were also among the leading primary
diagnoses, but were less likely to be made at ED visits for motor
vehicle traffic injuries compared with other injury-related ED visits.
NOTES: Figures are based on 2-year averages.
Categories based on the International Classification of Diseases, Ninth
Revision, Clinical Modification (ICD–9–CM). All percentages are
significantly different (p < 0.05) for motor vehicle traffic injuries compared with other causes of injury based on a two-tailed t test.
SOURCE: CDC/NCHS, National Hospital Ambulatory Medical Care Survey, 2010–2011.
Summary
This analysis of NHAMCS data indicates that in 2010–2011, there were
approximately 3.9 million ED visits for motor vehicle traffic injuries
annually, which accounted for 10.1% of all injury-related ED visits.
Visit rates were highest among those aged 16–24 and then declined with
age, with rates for persons aged 0–15 similar to those for persons aged
65 and over. Visit rates were also higher for non-Hispanic black persons
compared with non-Hispanic white and Hispanic persons. Although arrival
by ambulance occurred more than twice as often for ED visits for motor
vehicle traffic injuries than for other injury-related ED visits, the
percentage with a triage status of immediate or emergent was only
slightly higher, and there was no difference in the percentage admitted
to the hospital. Imaging was more frequently ordered or provided at ED
visits for motor vehicle traffic injuries compared with other
injury-related ED visits. Finally, sprains and strains of the neck and
back, contusion with intact skin surface, and spinal disorders accounted
for about one-half of all ED visits for motor vehicle traffic injuries.
Injury prevention objectives were recently outlined for Healthy
People 2020, and these include reducing motor vehicle crash-related
deaths and nonfatal motor vehicle crash-related injuries (
5).
Data on the rates and characteristics of ED visits for motor vehicle
traffic injuries can help inform public health efforts aimed at meeting
these objectives and continuing the progress made in improving motor
vehicle safety.
Definitions
Injury-related visit: A visit in which a first-,
second-, or third-listed external cause of injury, or first-, second-,
or third-listed reason for visit or diagnosis code that is injury- or
poison-related was recorded. Adverse effect and medical and surgical
misadventure or complication external cause-of-injury codes were
excluded; however, if these codes were present in combination with
other valid definitional codes, the visit was considered
injury-related. Diagnosis and external cause of injury were coded using
the
International Classification of Diseases, Ninth Revision, Clinical Modification (ICD–9–CM) (
6).
Visit for motor vehicle traffic injury: An injury-related visit with a first-listed external cause-of-injury code of 810–819 from the ICD–9–CM (
6). Specifically, these codes are:
- E810—Motor vehicle traffic accident involving collision with train
- E811—Motor vehicle traffic accident involving re-entrant collision with another motor vehicle
- E812—Other motor vehicle traffic accident involving collision with motor vehicle
- E813—Motor vehicle traffic accident involving collision with other vehicle
- E814—Motor vehicle traffic accident involving collision with pedestrian
- E815—Other motor vehicle traffic accident involving collision on the highway
- E816—Motor vehicle traffic accident due to loss of control, without collision on the highway
- E817—Noncollision motor vehicle traffic accident while boarding or alighting
- E818—Other noncollision motor vehicle traffic accident
- E819—Motor vehicle traffic accident of unspecified nature
References
- CDC. Ten significant public health achievements—United States, 2001–2010: Motor vehicle safety.
- CDC. Injury prevention & control: Motor vehicle safety.
- CDC. FastStats: Accidents or unintentional injuries.
- Naumann RB, Dellinger AM, Zaloshnja
E, Lawrence BA, Miller TR. Incidence and total lifetime costs of motor
vehicle-related fatal and nonfatal injury by road user type, United
States, 2005. Traffic Inj Prev 11(4):353–60. 2010.
- U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Healthy People 2020 topics and objectives: Injury and violence prevention
 . Washington, DC.
. Washington, DC.
- Centers for Medicare & Medicaid Services. International classification of diseases, ninth revision, clinical modification, 6th ed. DHHS Pub No. (PHS) 06–1260. 2006.
- NCHS. 2010 NHAMCS micro-data file documentation